Preppers: Protecting Yourself From Ebola Emerging Threats
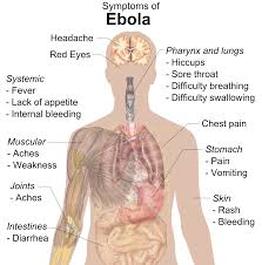
Preppers and Ebola: Protecting Yourself The current Ebola outbreak is the largest in history. It has caused more than 672 deaths and more than 1,200 infections in Guinea, Liberia and Sierra Leone, this according to the Centers for Disease Control and Prevention (CDC). To control the disease the chain of transmissions must be broken. While highly contagious the disease can be isolated, because you cannot become infected by simply breathing the virus in, it is not airborne, in other words. You have to have contact with an infected person’s bodily fluid, blood, feces, mucus, semen and even sweat. The mortality rates are high but keep in mind the medical facilities where the patients are now being treated are not as advanced, as they would be in the United States. If people became infected in the U.S. and received prompt medical treatment the mortality rate would likely drop to 50 percent or possibly lower. This is all speculation of course, because there has never been a reported case of one of the four deadly Ebola viruses in the United States. It is assumed that the medical professionals across the country have plans, and are ready to deal with the problem if it becomes a problem in the United States. However, this again is all speculation. Assume the Worst Experts and others claim the disease is just an airplane ride away from being in the United States and most claim it is not in the U.S. yet. Assume it is here however, because to assume otherwise, you would then not take the proper precautions when caring for someone with a high fever, who is vomiting and has severe stomach pains. These are just a few of the symptoms, and keep in mind influenza for example, may have the same symptoms to a certain extent, (refer to a previous article on Ebola symptoms and treatments). You as an individual should never treat anyone including family members, that you know or suspect has the virus without proper protection. Protection includes medical gloves, gowns, facemasks, shields and protective eyewear. First responders have to be particularly cautious when treating any victim for any reason, because a person can be a carrier and not show any symptoms. It is important that a travel history be obtained if possible. You must know where family members have traveled too. Even if they have not traveled to Africa, for example, interconnecting flights may have had an infected person on it. Medical experts claim that a person is not contagious or as contagious until the symptoms are full blown, but there is not a vaccine, which should tell you that the medical experts do not fully understand the virus, so never assume anything. Wear two pairs of protective gloves when handling needles. You should never reuse needles, but if you find you have to, the procedure for sterilization is to submerse the needles in hot soapy water to remove any obvious contaminates, such as blood mucus and so on. Once the needles have been cleansed of all blood or other fluids rinse well with clean water in a sterilized bowl or other container. Once rinsed draw undiluted chlorine bleach into the needles and let soak for 30 seconds. Expel the bleach safely, repeat the process, and let the needles air dry. This assumes the sodium hypochlorite (liquid chlorine) content is at least between 5.25 and 6 percent or higher. Elimination of All Microorganisms, Viral, Bacteria, and Fungal Through Sterilization Sterilization of hard, non-porous items can be accomplished by using high heat, an autoclave or steam sterilizer. Boiling heat-resilient items in water for 20 minutes will kill the Ebola virus as well. You can also use a bleach solution to kill the virus on hard surfaces, clothing and other items using a solution of 1:10 and a solution of 1:100. A 1:100 bleach solution is used to disinfect:
Washing your hands is always the first line of defense to protect yourself and others. Use bar soap that has been cut into chunks so you can use one piece and dispose of that piece. This prevents contamination of the entire bar of soap. Use one hand to scrub the hand, forearm of the opposite hand, and then switch using the other hand and then rinse well. Discard the piece of soap safely and always use a disposable one-time use towel or let the hands air dry. You cannot “catch” the virus by simply being in the same room with an infected person. However, you have to assume that if an infected person sneezes or coughs then micro mucus droplets can be transmitted through the air for short distances. If it is known or suspected a person has the disease use all available protection whenever in the same room. Bedding must be destroyed by incineration or proper procedures followed for sterilization and the same applies to the patients clothing. Physical barriers must be erected to isolate patients. This would include protective fencing, to prevent people from entering, or heavy sheets placed over doorways to alert others that a person is isolated. Signs alerting others should be placed were easily seen as well. Bathrooms used by the infected person must be isolated and not used by anyone else. Never enter a bathroom facility that an infected person has used without all protective clothing/gear in place. The best protection for individuals is of course isolation. Avoid crowds, do not fly and stay out of airport terminals. Once again, the virus is not floating in the air, so if you have not come in physical contact with an animal or a human that has the disease then you cannot catch the virus. It is likely but not proven that the virus is in the United States. Remember the mortality rate is directly related to the treatment of patients infected. Because there is no cure, treatment is therapeutic. Hydration levels must be maintained, blood pressure monitored closely and most patients have to be treated for secondary infections caused by the virus. Excessive internal and external bleeding is common and a common cause of death from the virus. This must be treated promptly by professionals. Do not attempt to treat anyone at home that you suspect has the virus. The information provided is for informational purposes only and is not to be considered medical advice. CDC. (2014). Retrieved 2014, from http://www.cdc.gov/vhf/ebola/ __________________________ 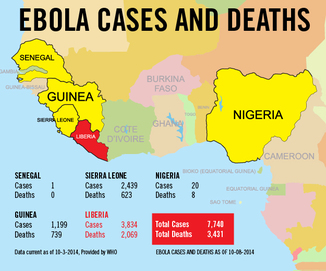
HERE'S WHERE EBOLA COULD SPREAD NEXT
Air-travel map shows probable paths of virus Published: 3 hours ago JEROME R. CORSI NEW YORK – An interactive map plotting the airline flights originating in Monrovia, Liberia, makes clear why international health officials are concerned Europe is the next place where the Ebola virus could spread. Already, one case of Ebola has been confirmed in Spain, and the Independent newspaper in the United Kingdom is reporting scientific analysis concluding there is a 75 percent chance Ebola will hit France by Oct. 24 and a 50 percent chance it will hit Britain by the end of the month.. The interactive air-travel map</b? shows Europe is the most common transit point for international travelers traveling from Liberia to the U.S. Flights from Monrovia, Liberia, easily connect with international flights to Lisbon, Madrid, Paris, Brussels, Frankfurt, Bologna, Rome and London. Flights from Brussels regularly connect to New York’s JFK, Dallas-Fort Worth and Chicago in the United States along with destinations such as Tel-Aviv, Montreal, Toronto and New Delhi. How easy is it for someone from Liberia that is already infected with Ebola to leave the country by air? As demonstrated by the case of Thomas Eric Duncan – the Liberian infected with Ebola who died this week in a Dallas hospital – the authorities in Monrovia screening departing passengers have no way to know if someone claiming to have had no contact with Ebola-infected individuals is lying. Furthermore, since the disease can take up to 21 days to incubate before symptoms manifest, a person infected with Ebola could easily pass through security in Monrovia undetected. How easy is it to depart from Monrovia to travel internationally? Three flights a day depart Monrovia for Casablanca, the main connecting airport for European flights. One flight each day flies non-stop from Monrovia to Brussels. As the interactive map demonstrates, there are direct flights connecting Casablanca with New York’s JFK International Airport, just as there are flights from Dakar, Senegal, to Dulles International in Washington, D.C., as well as to JFK. As WND reported Oct. 2, there are hundreds of ways to fly from Liberia to the United States and connect to every airport in the country. A spreadsheet listing connecting flights from Monrovia through Casablanca shows more than 100 destinations, including cities in Africa, the Middle East, South America, Russia, Europe and the United States. Both the United Nations’ World Health Organization and the Centers for Disease Control and Prevention in Atlanta continue to insist a restriction on air travel from West Africa would only increase the spread of the disease. The agencies contend it would make it more difficult for international health authorities to get qualified medical personnel and supplies to the affected nations. WND has also reported an international team of scientists argued a reduction in airline travel of as much as 80 percent would only delay the international spread of Ebola by three to four weeks at most. Interactive Map by Jeff Eisman – Geographic Information System – GIS – Consultant – [email protected]. Read more at... _________________________ |

STUDY: 31-DAY QUARANTINE REQUIRED FOR EBOLA
Current government assumptions could expose public to disease Published: 3 hours ago JEROME R. CORSI NEW YORK – A recently published scientific study has concluded a 21-day quarantine period for Ebola is not enough. Challenging the scientific basis for the World Health Organization and the Centers for Disease Control and Prevention recommendation, the study concludes 31 days may be required to have a 95 percent certainty a person has not contacted Ebola. Dr. Charles Haas of the Department of Civil, Architectural and Environmental Engineering at Drexel University is the author the study, “On the Quarantine Period for the Ebola Virus,” published Oct. 13 in the scientific journal PLOS: Currents Outbreaks. He has concluded a 21-day quarantine period for Ebola may result in the release of individuals who still have up to a 12 percent risk of having the disease. “While the 21-day quarantine value currently used may have arose from reasonable interpretation of early outbreak data, this work suggests a reconsideration is in order and that 21 days may not be sufficiently protective to public health,” Haas concluded, suggesting the WHO recommendation was based on faulty data analysis. Examining more recent disease data from the current West African outbreak as well as from other outbreaks, Haas suggests a 31-day quarantine period may be necessary. Haas criticizes the WHO for relying on potentially flawed data, noting “the precise origin of this assessment is unclear.” It appears the U.N. agency relied primarily on studies of the 1976 Zaire outbreak or the 2000 Uganda outbreak, “both of which reported (without detailed analysis) a maximum observed incubation of 21 days.” As for the origin of the WHO’s current 21-day quarantine recommendation, Haas cited a study the WHO published in September. It was based only on an analysis of data from the first nine months of the current Ebola outbreak in West Africa. It reported an average incubation period of 11.4 days with an upper 95th percentile of 21 days. Haas’ analysis, however, was based on more recent data from the current West Africa outbreak, as well as a larger dataset of cases from the 1995 outbreak in the Congo that proved a quarantine of 21 days was too short. The 1995 data found 12 percent of the Ebola-exposed patients released developed the disease and become contagious sometime after 21 days. Haas stressed that analysis of the more extensive patient database set from the 1995 Congo outbreak suggests a quarantine time of 31 days is required to reach the upper 95th percentile of the Ebola incubation time distribution. A summary of the research published on the Drexel University website said, “Haas, who has extensive background in analyzing risk of transmitting biological pathogens, explains that these quarantine periods must be determined by looking at the cost of enforcing the quarantine versus the cost of releasing exposed individuals.” The note concludes, “Obviously, with more contagious and potentially deadly diseases the cost of making a mistake on the short side when determining a quarantine is extremely high.” Haas said it’s clear that pathogens with a high degree of transmissibility and/or a high degree of severity, should have a longer quarantine time. “The purpose of this paper is not to estimate where the balancing point should be, but to suggest a method for determining the balancing point,” he said. As WND reported, the Obama administration has stated U.S. health-care workers returning home after treating Ebola-infected patients in West Africa should be treated as “heroes” rather than be punished by being placed in quarantine after traveling by air from West Africa to the United States. On Monday, the CDC redefined previously published health-care protocols recommending state health officials should not mandate a 21-day quarantine for U.S. citizens, including health-care workers, upon their return to the United States after exposure to Ebola in West Africa. Instead, U.S. citizens, including health-care workers, exposed to Ebola in West Africa should be placed under “active monitoring,” requiring them to make daily telephone calls to state health officials reporting possible any symptoms of Ebola that may develop, including fever, in the first 21 days after returning home. WND has also reported the Pentagon decision to place 11 U.S. soldiers returning from Liberia in 21-days quarantine at a U.S. military base in Vicenza, Italy, represents an apparent policy conflict with the “active monitoring” policy. Read more at __________________________ 
CARIBBEAN, SOUTH AMERICAN COUNTRIES CLOSE BORDERS TO COMBAT EBOLA
by JORDAN SCHACHTEL 17 Oct 2014 107POST A COMMENT Colombia, Jamaica, Guyana, and Trinidad and Tobago have all announced travel bans as Ebola concerns grow.Colombian authorities announced that anyone entering their country from Ebola-stricken countries will face heavy scrutiny. Colombia’s National Health Institutes have said they developed a questionnaire to determine who should be under suspicion of potentially having contact with Ebola. Colombian newspapers have reported that some have already been detained due to the newly instituted executive actions. Fernando Ruiz, Colombia’s vice minister of health, said of the reports, “The cases are not suspicious. They are simply people who have traveled to places where Ebola is present. That is the reason for their medical observation.” He added, “The three cases are not under strict surveillance. Their temperature is measured two times a day for 21 days. At this moment, we are not alerted or worried. The individuals seem healthy. Two of them already completed their observation period.” The Jamaican government on Thursday authorized an immediate travel ban against persons traveling from the Ebola-affected nations of Liberia, Sierra Leone, and Guinea. Jamaican authorities said that anyone who has traveled into the three West African countries in the last twenty-eight days is forbidden from entering their country. Jamaican citizens who have traveled to the African lands within the past twenty-eight days will be subject to quarantine. On Thursday, the government of Trinidad and Tobago banned entry to visitors arriving from several African countries which have had documented Ebola infections. Trinidad and Tobago Health Minister Dr. Fuad Khan said that anyone arriving from Liberia, Sierra Leone, Guinea, Democratic Republic of Congo, or Nigeria will be forbidden from entry. Citizens who have traveled to those countries within the past six weeks will be quarantined for 21 days, the Health Ministry reported. The government of Guyana also announced that its diplomatic services overseas were told not to extend visas to individuals from the Ebola-affected West African nations. U.S. President Barack Obama announced that he disagrees with a travel ban to and from Ebola-stricken nations and told reporters that “a flat-out travel ban is not the way to go.” __________________________ 
Oct 19th
U.S. ARMY WARNS OF POTENTIAL 'AIRBORNE' EBOLA Virus could be transmitted by means other than contact Published: 3 days ago JEROME R. CORSI NEW YORK – While Centers for Disease Control and World Health Organization officials continue to insist Ebola cannot be transmitted by air from one person to another, an Army manual clearly warns the virus could be an airborne threat in certain circumstances. The handbook published by the U.S. Army Medical Research Institute of Infectious Diseases, USAMRID, titled “USAMRID’s Medical Management of Biological Casualties Handbook,” is now in its seventh edition. The most recent edition was published in 2011, with more than 100,000 copies distributed to military and civilian health-care providers around the world. On page 117 of the handbook, in a chapter discussing “Viral Hemorrhagic Fever” (VHF), a category of viruses that includes Ebola, USAMRID says: “In several instances, secondary infections among contacts and medical personnel without direct body fluid exposure have been documented. These instances have prompted concern of a rare phenomenon of aerosol transmission of infection.” Page 117 continues to specify: “Therefore, when VHF is suspected, additional infection control measures are indicated.” USAMRID recommends the patient should be hospitalized in a private room with an adjoining anteroom to be used for donning and removing protective barriers, storage of supplies and decontamination of laboratory specimen containers. WND recently reported the World Health Organization, in a largely overlooked media advisory email, admitted there are some circumstances in which the current strain of Ebola in West Africa can be transmitted through coughing or sneezing. “Theoretically, wet and bigger droplets from a heavily infected individual, who has respiratory symptoms caused by other conditions or who vomits violently, could transmit the virus – over a short distance – to another nearby person,” the WHO Ebola situation assessment said. “This could happen when virus-laden heavy droplets are directly propelled, by coughing or sneezing (which does not mean airborne transmission) onto the mucus membranes or skin with cuts or abrasions of another person.” Air-purifying equipment The USAMRID handbook recommends that for all VHF patients with significant cough, hemorrhaging or diarrhea, the hospital room should be a “negative-pressure isolation room” with six to 12 air exchanges, adequate to pump air out of the hospital room on a constant basis through bio-filters. To make the point about airborne transmission of VHF viruses, including Ebola, USAMRID says all persons entering the patient’s room should wear double gloves, impermeable gowns with leg and shoe coverings for contact isolation, eye protection and HEPA (N-95) masks or positive-pressure air-purifying respirators (PARRS). In the absence of a large, fixed medical-treatment facility, or in the event of an overwhelming number of casualties when isolation rooms may not be available for all patients, USAMRID recommends that at a minimum, VHF patients should stay together in “a ward with an air-handling system separate from the rest of the building when feasible.” The manual notes that clinical laboratory personnel are “at significant risk for exposure” and should employ a bio-safety cabinet when available, with barrier and respiratory precautions when handling specimens. ‘We have to consider the possibility’ Dr. David Sanders, a top Ebola virologist and Purdue University professor of biological science appeared on Fox News on Monday to discuss his research suggesting Ebola can be an airborne virus. “Our own research shows that Ebola Zaire enters human lung cells from the airway side. So it has the inherent capacity to enter the lung from the airway,” he said. “I’m not saying that there’s any evidence that the current spread is due to anything but bodily fluid contact, but we have to consider the possibility that it can enter through an airway route.” Read more at __________________________ |
 (Photo: Mike DuBose, United Methodist News Service, via European Pressphoto Agency) (Photo: Mike DuBose, United Methodist News Service, via European Pressphoto Agency)
Nebraska patient case raises questions about Ebola test
Liz Szabo, USA TODAY 3:44 p.m. EST November 17, 2014 Dr. Daniel Johnson of University of Nebraska Medical Center confirmed Monday that Dr. Salia, a surgeon who tested positive for Ebola in Sierra Leone, died after going into cardiac arrest. VPC The death of physician Martin Salia from Ebola has raised questions about the tests and drugs used in the disease. Salia, a surgeon who was flown from Sierra Leone to Omaha's Nebraska Medical Center Saturday, had two negative tests for Ebola before testing positive. He arrived in Omaha on the thirteenth day of his illness, said Phil Smith, medical director of the Nebraska hospital's biocontainment unit, one of four around the USA designed for the most dangerous infectious diseases. Salia is the 10th person with Ebola treated in the USA. While all eight Americans have survived, both patients from Africa -- including Liberian national Thomas Eric Duncan -- have died. Although Ebola tests are generally considered accurate, they may produce false negative results early in a person's infection, when levels of the virus are still low, says Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases. The test isn't sensitive enough to detect very small amounts of virus. That's why people who suspect they could have Ebola -- because they have symptoms and may have been exposed to the virus -- should be retested again in 48 to 72 hours, Fauci says. Guidelines from Doctors Without Borders note that, "false negative results can occur in the first three days of symptoms when the viral load is low. If the disease is suspected and the result is negative, the test needs to be repeated on or after the fourth day of symptoms." Fauci says false negative results don't pose a major public health risk. That's because people with low levels of virus aren't very contagious. People generally become more contagious as the level of virus rises, later in the illness. That puts hospital workers at greater risk than the average person in the community. Even a patient who has begun to feel sick is not likely to spread the disease to others until the patient begins to lose bodily fluids, such as through blood, vomit and diarrhea, Fauci says. In addition to supportive care in the intensive care unit, Salia received two experimental therapies -- a blood donation from someone who survived Ebola and the drug ZMapp. Hospital officials declined to reveal which Ebola survivor provided the blood. Salia is the first Ebola patient to receive ZMapp in the USA since August, when the drug was given to physician Kent Brantly and missionary Nancy Writebol. A handful of Ebola patients in other countries also received the drug, which isn't yet approved. An Aug. 12 statement on the web site of ZMapp's maker, Mapp Biopharmaceutical of San Diego, says that supplies of the drug have been exhausted. The drug takes several months to produce, using tobacco plants. An undated United Methodist News Service handout shows Dr. Martin Salia at United Methodist Kissy Hospital outside Freetown, Sierra Leone.(Photo: Mike DuBose, United Methodist News Service, via European Pressphoto Agency) But when the hospital contacted Mapp Biopharmaceutical, the company was able to send a dose, said Chris Kratochvil, the associate vice chair for clinical research at the University of Nebraska Medical Center. "We don't have any recognized supplies of ZMapp," Fauci said. "It's obvious that somewhere, somehow, people have a dose or two stowed away. When people get it, I'm not sure where they get it from." Nebraska doctors said they used a variety of therapies to try to save Salia, who was unresponsive and in kidney failure and respiratory failure when he arrived Saturday. Those methods included kidney dialysis and a breathing machine. Doctors gave him two powerful drugs to raise his blood pressure, which was collapsing. Those efforts came too late in Salia's illness. He died 36 hours of cardiac arrest after arriving in Omaha. "The earlier you start supportive care, the better," Smith said. Thomas Geisbert, a professor of microbiology and immunology at the University of Texas Medical Branch, has researched experimental Ebola therapies in animals for years. When getting therapy to people infected with the disease, "every day matters; every hour matters," he says. Ebola has killed more than 5,000 people, largely in Sierra Leone, Liberia and Guinea. A separate Ebola outbreak in the Democratic Republic of Congo, which began in August and is unrelated to the West African outbreak, is now under control. There have been new cases since Oct. 4, according to Doctors Without Borders. __________________________ Certitudinous
Thank you Kent Lamberson Obama Plans to Let Ebola-infected Foreigners Into U.S. for Treatment
OCTOBER 17, 2014 Washington, DC – Judicial Watch has learned that the Obama administration is actively formulating plans to admit Ebola-infected non-U.S. citizens into the United States for treatment. Specifically, the goal of the administration is to bring Ebola patients into the United States for treatment within the first days of diagnosis. It is unclear who would bear the high costs of transporting and treating non-citizen Ebola patients. The plans include special waivers of laws and regulations that ban the admission of non-citizens with a communicable disease as dangerous as Ebola. One source tells us that the Obama administration is keeping this plan secret from Congress. The source is concerned that the proposal is illegal; endangers the public health and welfare; and should require the approval of Congress. Read more about Ebola ___________________________ 
Politicizing a Plague
By Alan Caruba October 15, 2014 If President Obama does not want the Ebola virus to kill Americans, why has his administration done nothing to restrict any flights from Liberia, Guinea, and Sierra Leone, the hot spots in Africa where it appears the virus is spreading? One of the reason flights from Liberia were not stopped, we have been told, was the historical link of the U.S. with that nation, founded as a place freed slaves could migrate. That is no excuse in the face of the threat of a single Liberian with Ebola getting off a flight in any U.S. airport. The decision not to stop flights has nothing to do with health and everything to do with politics, Obama’s far left ideology, and his dislike for America that has been on display for anyone paying any attention. It has driven every decision Obama has made since first taking office. The White House has decided that stopping flights would heighten public concerns, possibly creating an aura of panic. This is a very bad, very lethal decision. It demonstrates the indifference to facts and to common sense for which the White House is now famous. Every poll demonstrates that Americans want our borders protected and access from West Africa denied. It is likely that the White House wants to tamp down any sense of heightened public concern until the midterm elections on Nov. 4. Then add to that the criminal lack of truthfulness that has accompanied anything affecting this White House has done from Benghazi to setting free five Taliban generals in exchange for someone likely to be deemed a deserter from the U.S. Army. Director of the Centers for Disease Control (CDC), Dr. Thomas FriedmanWhen the Director of the Centers for Disease Control (CDC), Dr. Thomas Friedman, became the focus of news media inquiries regarding the virus, it was clear that he did not have any greater knowledge of the problem, other than the scope of its threat, than anyone else. Indeed, within a week of his first press conference, he said that the CDC and U.S. medical community needed to come up with a whole new approach to Ebola. When Thomas Duncan, the Liberian in whom the virus was not initially detected died, we were treated to scenes of intensive decontamination efforts at the Dallas hospital, but a nurse who treated him became the first U.S. victim and Dr. Friedman was quick to blame a “protocol breach” as the likely reason. Now a second nurse has Ebola. The likely reason can be found in the fact that thousands of people die every year from viruses and infections they acquire at a hospital. The first and likely the second nurse wore protective outfits from top to bottom while dealing with Duncan. In Africa, the earliest victims have been the doctors and hospital staff tending those with Ebola. Any U.S. medical personnel returning from Africa should be quarantined after they arrive. The President has dispatched more than 4,000 military personnel to Liberia and their quarantine should be far longer than the 21 days we keep hearing about. We are now hearing it should be up to 40 days. Notion that airport staff has any capacity at all to spot someone with Ebola is ludicrousThe notion that airport staff has any capacity at all to spot someone with Ebola is ludicrous, yet we are being treated to the charade of passengers having a device waved over them to detect a fever. All this is a political approach rather than a medical one. It is political theatre. One example of this was a statement by Dr. Francis Collins, the head of the National Institutes of Health, who blamed the lack of funding the NIH has received for research, including vaccinations for infectious diseases. He noted that the NIH has been working on Ebola vaccines since 2001, but does it strike anyone as odd that in all the time since then nothing has been developed? In fairness, though, the NIH budget has declined 23% over the past decade. The current budget, however, is $29.31 billion. That is a substantial amount. Congress represents more politics. Dr. Collins remarked that it did not appear “enthusiastic” about passing an emergency supplemental appropriation. For those in government the only answer to any problem is to throw more money at it. Worse, a Democratic Party advertisement even claimed that the Ebola threat is due to Republican cuts in funding of healthcare research, but those cuts were bipartisan by virtue of the sequestration limits imposed. Not mentioned was an Obama administration decision to abandon a set of regulations which the CDC considered essential to prevent international travelers from spreading deadly diseases inside the U.S. At this point, the question is why? So far Ebola has been located in West Africa, but in this world of global air travel, but without rigid restrictions it is only a matter of time before it begins to show up elsewhere including here again. When that happens you can point a finger at Barack Hussein Obama who thinks it’s more important to have good relations with Liberia than it is to shut down any possibility that an African or anyone else at risk of having Ebola will arrive on our shores. At that point, however, it will be too late. © Alan Caruba, 2014 Scroll down this page for Disqus Comments | 0 Comments--Comment hereAlan has a daily blog called Warning Signs. Alan can be reached at [email protected] __________________________ |
